













 10 / 21
10 / 21

Duckett Creek Sanitary District
9
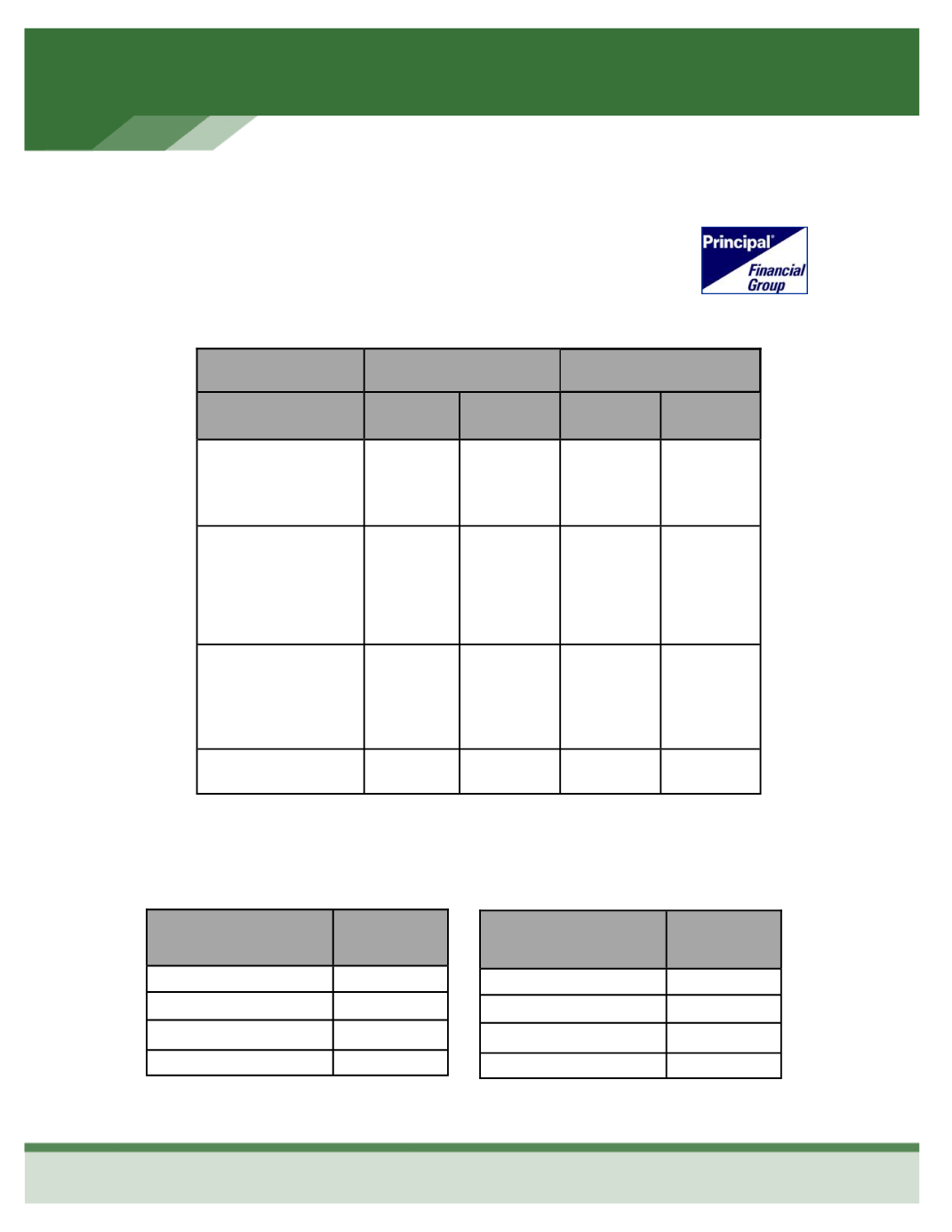
Enhance Your Smile with Dental Coverage
PRINCIPAL
High Plan
Low Plan
Benefits
In-Network
Out-of-
Network
In-Network
Out-of-
Network
Deductible
Individual
Family
$50
$150
$50
$150
$50
$150
$50
$150
Coinsurance
Diagnostic
Basic
Major
100%
90%
60%
100%
80%
50%
100%
80%
50%
80%
50%
25%
Orthodontia
(Adult & Child)
50% up to
$1,000
Lifetime
Maximum
50% up to
$1,000
Lifetime
Maximum
50% up to
$1,000
Lifetime
Maximum
50% up to
$1,000
Lifetime
Maximum
Annual Maximum
$1,000
$1,000
$1,000
$1,000
HIGH PLAN
Employee
$3.33
Employee & Spouse
$11.66
Employee & Child(ren)
$15.98
Employee & Family
$25.82
Employee Cost Per Bi-Monthly Pay Period
LOW PLAN
Employee
$0
Employee & Spouse
$4.95
Employee & Child(ren)
$7.88
Employee & Family
$13.77