















 4 / 13
4 / 13

Boyle Brasher LLC
2016 Annual Enrollment
2016 Page 4
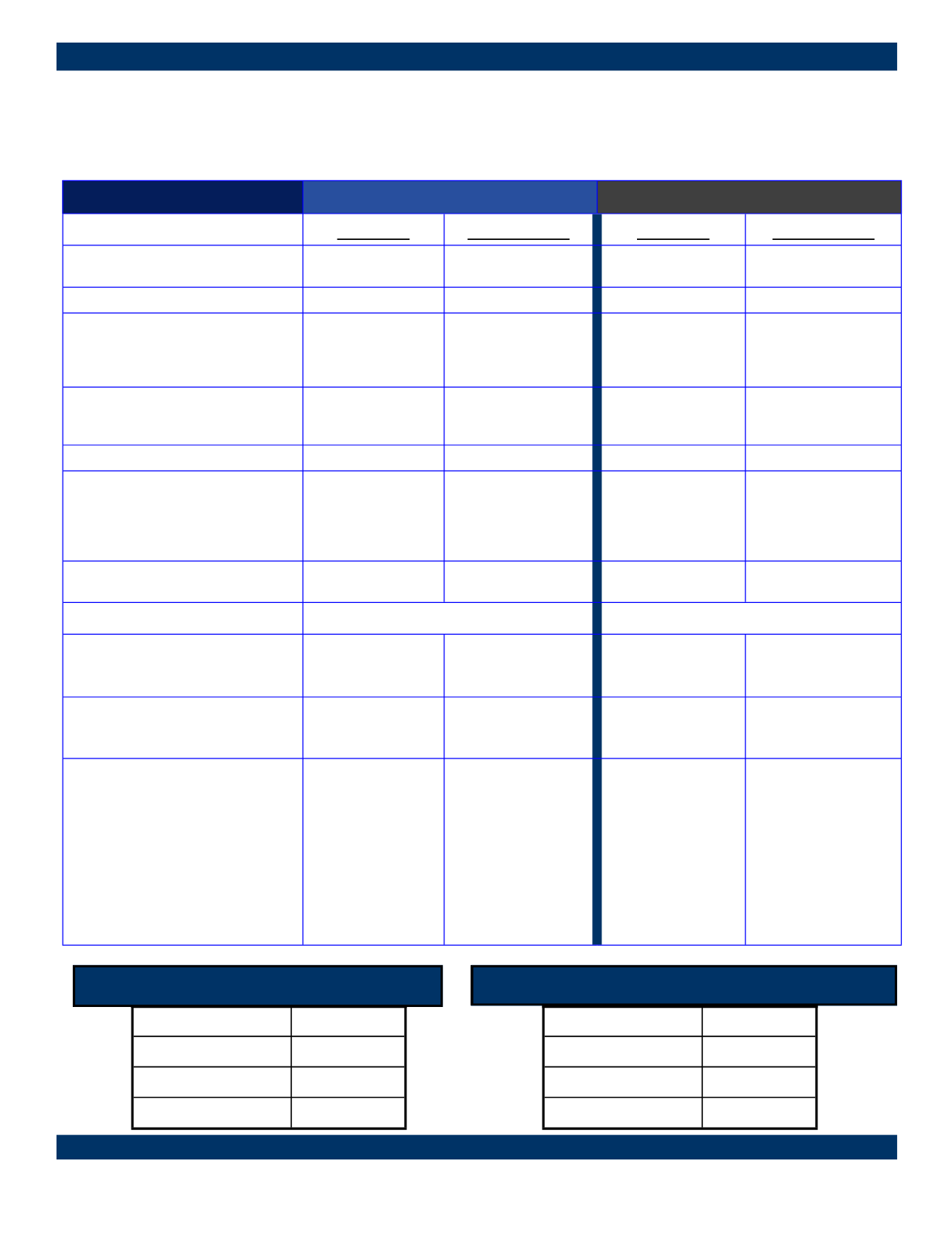
Your Medical Insurance Plan Options
Anthem BCBS - Plan Designs
Features
Traditional PPO Plan 4 / Rx AL
Lumenos EI / Rx AH
Qualified High Deductible H S A Plan
In-Network
Out-of-Network
In-Network
Out-of-Network
Deductible
(Individual / Family)
$1,000 / $3,000
$3,000 / $6,000
$3,000 / $6,000
$6,000 / $12,000
Coinsurance
90%
70%
100%
70%
Out-of-Pocket Maximum
(Individual / Family)
Includes Deductible, Coinsurance &
Co-Pays
$4,000 / $8,000
$8,000 / $16,000
$4,000 / $8,000
$12,000 / $24,000
Office Visit
(Primary Care physician / Specialist)
$25 / $50 Co-Pay
Ded., & Coinsurance
Ded., & Coinsurance
Ded., & Coinsurance
Preventive Care
100%
Ded., & Coinsurance
100%
Ded., & Coinsurance
Major Diagnostics:
(MRI, CT, PET, MRI, MRA)
Ded., & Coinsurance
Ded., & Coinsurance
100% after deducti-
ble
70% after deductible
Urgent Care
$75 Co-Pay
Ded., & Coinsurance
Ded., & Coinsurance Ded., & Coinsurance
Emergency Room
$250 Co-Pay, then 90% Coinsurance
Ded., & Coinsurance
Outpatient Surgery
Ded., & Coinsurance Ded., & Coinsurance
Ded., & Coinsurance Ded., & Coinsurance
Inpatient Hospital Services
Ded., & Coinsurance Ded., & Coinsurance
Ded., & Coinsurance Ded., & Coinsurance
Prescription Drug
Retail (at Participating Pharmacies)
Mail Order (90-Day Supply)
$10/$35/$60/25% to
$200 Max.
$10/$90/180/25% to
$200 Max.
Ded., then:
$10/$35/$60/25% to
$200 Max.
$10/$90/180/25% to
$200 Max.
50%, Min $60
Not Covered
Ded., then:
50%, Min $60
Not Covered
TRADITIONAL PPO EMPLOYEE CONTRIBUTIONS
QUALIFIED HIGH DEDUCTIBLE EMPLOYEE CONTRIBUTIONS
Employee Only
$2.00
Employee & Spouse
$647.19
Employee & Children
$621.89
Employee & Family
$1,267.07
Employee Only
$2.00
Employee & Spouse
$432.74
Employee & Children
$415.86
Employee & Family
$846.59