













 5 / 18
5 / 18

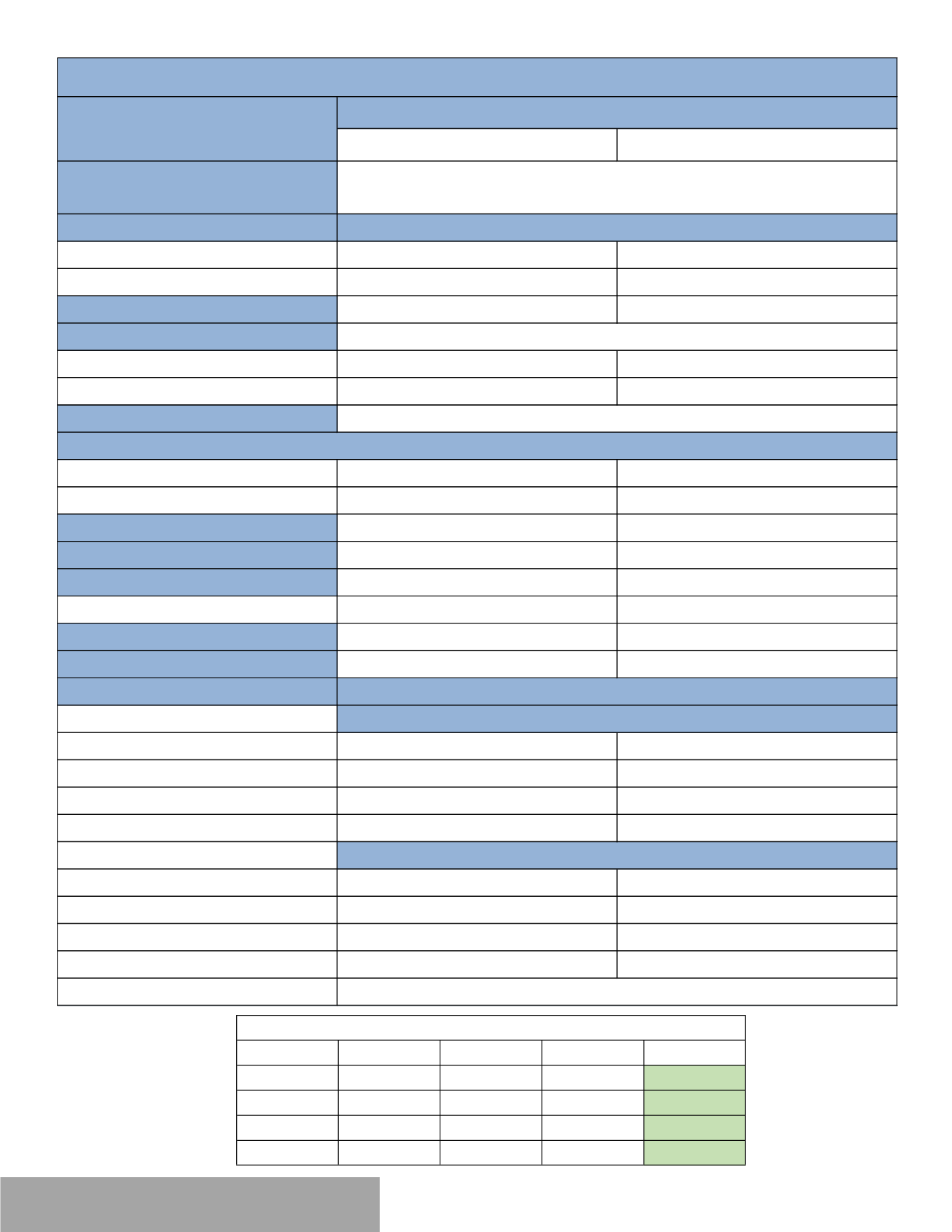
In-Network
Out-of-Network
Overview
Deductible
Individual
$2,000
$4,000
Family
$4,000
$8,000
Coinsurance
Plan pays 70% after Deductible
Plan pays 60% after Deductible
Out of Pocket Maximum
Individual
$6,600
$12,000
Family
$13,200
$24,000
Lifetime Maximum
Primary Care Physician
$35 Copay
Plan pays 60% after Deductible
Specialist
$70 Copay
Plan pays 60% after Deductible
Preventive Care Services
Plan pays 100%
Plan pays 60% after Deductible
Inpatient
Plan pays 70% after deductible
Plan pays 60% after Deductible
Outpatient Surgery
Plan pays 70% after deductible
Plan pays 60% after Deductible
Emergency Room
$500 Copay
$500 Copay
Urgent Care
$100 Copay
Plan pays 60% after Deductible
Prescription Drugs
Retail Pharmacy
(31 days)
Tier 1
$10 Copay
$10 Copay
Tier 2
$35 Copay
$35 Copay
Tier 3
$60 Copay
$60 Copay
Tier 4
$100 Copay
$100 Copay
Mail Order Pharmacy
(90 days)
Tier 1
$30 Copay
Not Covered
Tier 2
$105 Copay
Not Covered
Tier 3
$180 Copay
Not Covered
Tier 4
$300 Copay
Not Covered
Specialty Drugs
Includes Deductible/Coinsurance/Copays
Medical Coverage - United Healthcare
Type of Plan
Choice Plus High Plan 8BF
May use both In-Network and Out-of-Network providers
Use Network providers and receive the In-Network level of benefits
Use Non-Network providers receive a lower level of benefits and you may be subject to Balance Billing.
Unlimited
Office Visits
T1 $10 - T2 $100 - T3 $200 - T4 $300
Option 3 $2000
70%
(8B-F)
Medical
JDC
EE
Per Payroll
EE
$438.36
$ 173.97
$264.39
$122.03
EE+SP
$920.55
$ 173.97
$746.58
$344.58
EE+CH
$832.89
$ 173.97
$658.92
$304.12
FAMILY
$1,315.08
$ 173.97
$1,141.11
$526.67