














 2 / 12
2 / 12

E
MPLOYEE
C
ONTRIBUTIONS
You may select a provider from the following networks:
www.aetna.comor call 1-800-872-3862 or the Member Services number on your ID card
For more online services and tools:
Register on
www.aetnanavigator.comM
EDICAL
B
ENEFITS
D
ESCRIPTION
B E N E F I T S P L A N O V E R V I E W
P A G E 2
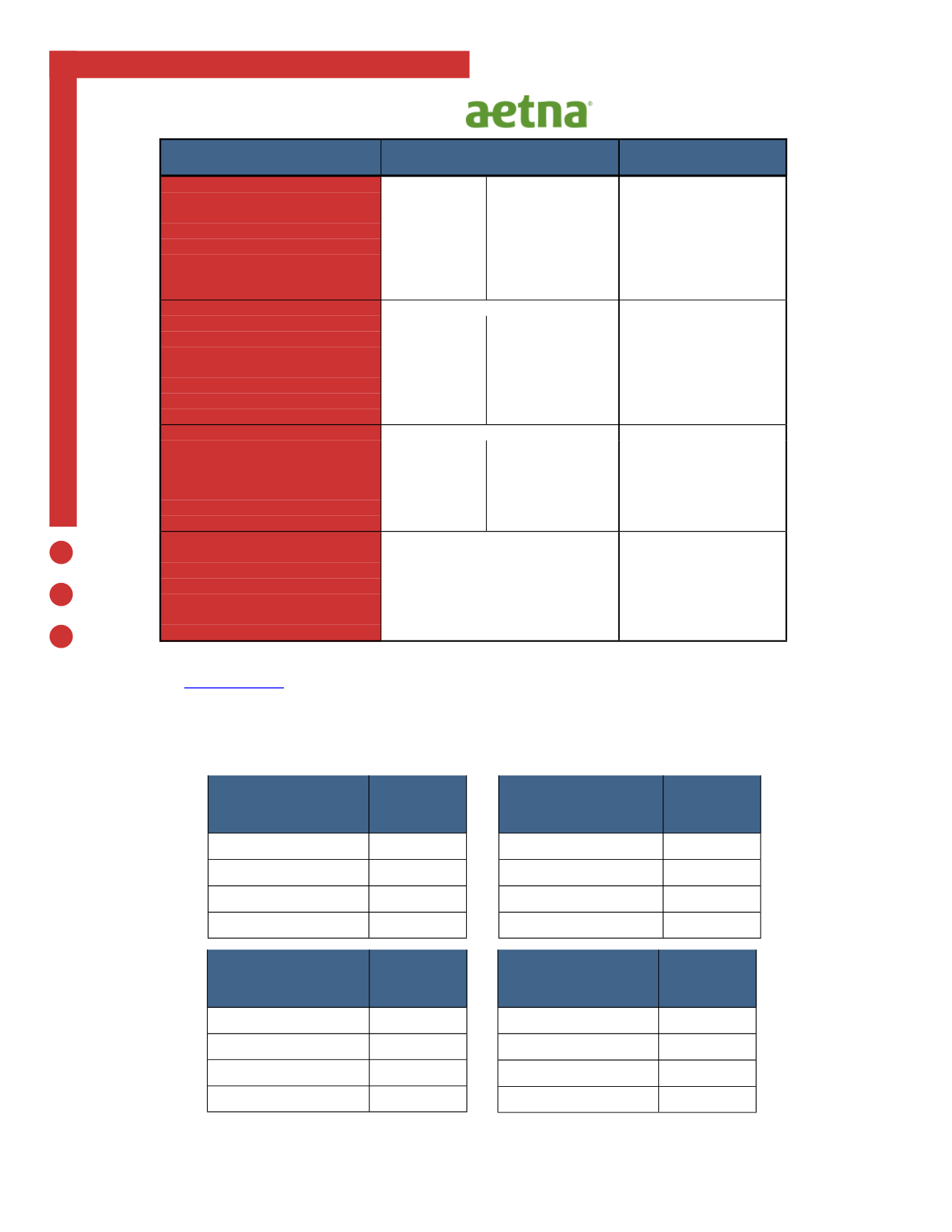
Aetna IH & Non-IH
PPO 1500 HSA
Employee
Bi-Monthly
Cost
Employee Only
$27.76
Employee + Spouse
$261.14
Employee + Child(ren)
$233.70
Family
$429.10
Dental
Employee
Bi-Monthly
Cost
Employee Only
$0.00
Employee + Spouse
$15.51
Employee + Child(ren)
$22.97
Family
$42.74
Vision
Employee
Bi-Monthly
Cost
Employee Only
$0.00
Employee + Spouse
$4.04
Employee + Child(ren)
$2.80
Family
$7.23
Aetna IH & Non-IH
Open HMO 2500 HSA
Employee
Bi-Monthly
Cost
Employee Only
$13.40
Employee + Spouse
$119.35
Employee + Child(ren)
$89.10
Family
$239.25
Plan Design
Aetna IH & Non-IH
Aetna IH & Non-IH
PPO 1500 HSA
Open HMO 2500 HSA
Deductible (Policy Year):
In Network
Out of Network
In Network Only
- Single
$1,500
$3,000
$2,500
- Family
$3,000
$6,000
$5,000
Out of Pocket Maximum (Policy Year):
- Single
$3,000
$6,000
$5,000
- Family
$6,000
$12,000
$6,850
Coinsurance:
Copays
70% / 30% Allowed
Benefit
Copays
Office Visits:
Deductible First, then;
Deductible First, then;
- Primary Care Physician
$20 Copay
30% Allowed Benefit
$30 Copay
- Specialist
$40 Copay
30% Allowed Benefit
$50 Copay
- Lab and x-ray (free standing)
$40 Copay
30% Allowed Benefit
$50 Copay
Routine Coverage:
- Well Baby
Covered in Full 30% Allowed Benefit
Covered in Full
- Adult
Covered in Full 30% Allowed Benefit
Covered in Full
Deductible waived for Preventive
Hospitalization:
Deductible First, then;
Deductible First, then;
- Inpatient
$500 / Admission 30% Allowed Benefit $300 copay per day to a max
copay of $1500 per
admission
- Outpatient
$300 Copay
30% Allowed Benefit
$200 Copay
- Accident/Medical Emergency
$200 Copay
Same as In network
$200 Copay
- Urgent Care
$75 Copay
30% Allowed Benefit
$75 Copay
Prescription Drugs:
Integrated medical and rx
Integrated medical and rx
- Generic
$10 Copay
$10 Copay
- Brand (Formulary)
$35 Copay
$35 Copay
- Brand (Non-Formulary)
$60 Copay
$60 Copay
- Specialty Drugs
$200 Copay
$200 Copay
- Mail Order
2 x Copay
2 x Copay
Lifetime Maximum
Unlimited
Unlimited