
















 9 / 38
9 / 38

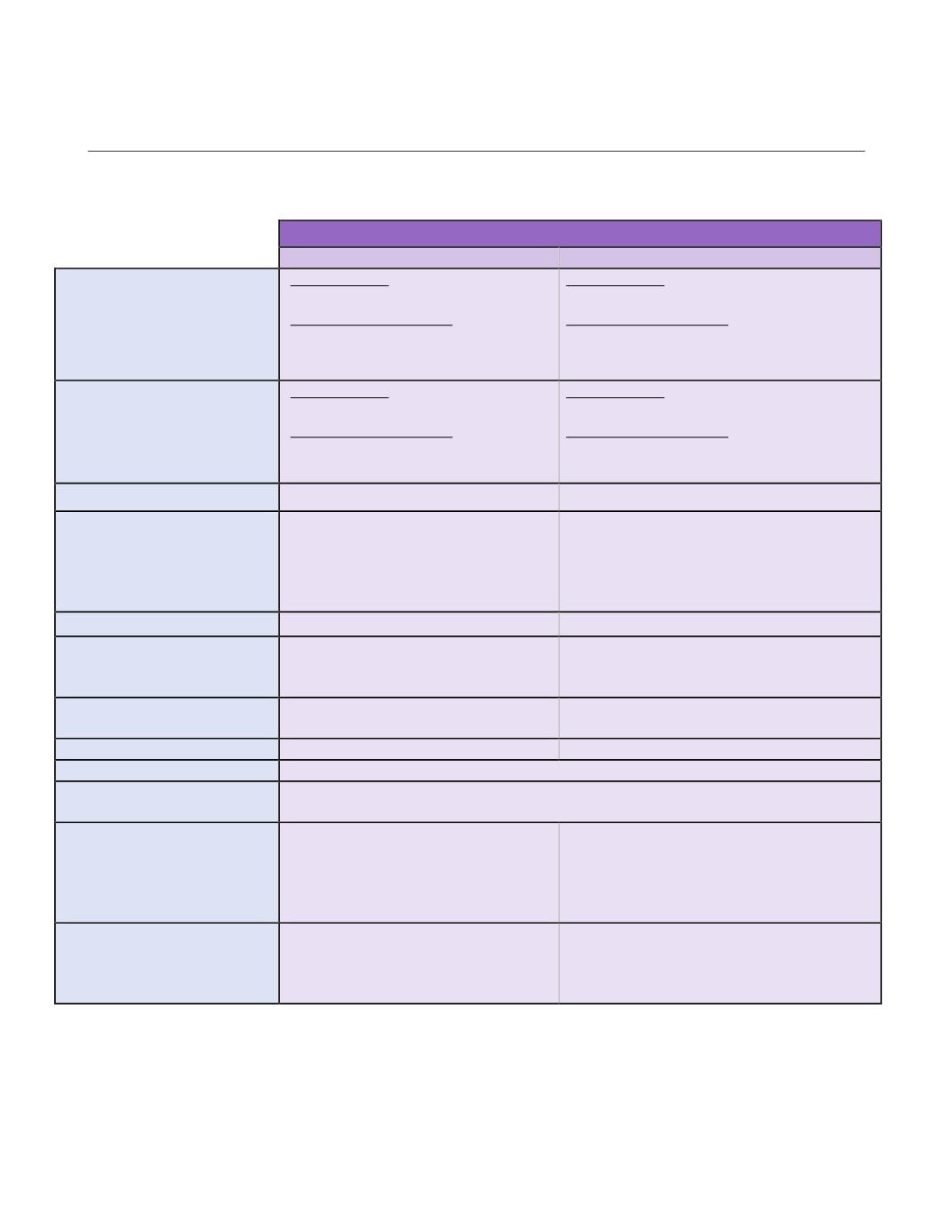
MEDI CAL , CONT I NUED
HDHP Plan
Blue Shield HDHP
In-Network
Out-of-Network
Plan Year Deductible
1
Individual
Family
Employee only:
$2,250
Employee + Dependents:
$2,600 / Individual
$4,500 / Family
Employee only:
$2,250
Employee + Dependents:
$2,600 / Individual
$4,500 / Family
Plan Year Out-of-Pocket Max
2
Individual
Family
Employee only:
$3,000
Employee + Dependents:
$3,000 / Individual
$6,000 / Family
Employee only:
$6,000
Employee + Dependents:
$6,000 / Individual
$12,000 / Family
Preventive Services
No Charge
Not Covered
Office Visits
Primary Care Physician (PCP)
Specialist
Chiropractic Services
(limited to 12 visits per year)
20% after deductible
20% after deductible
20% after deductible
50% after deductible
50% after deductible
50% after deductible
Urgent Care
20% after deductible
50% after deductible
Lab and X-ray
CT, MRI, PET scans
Other labs and x-ray tests
$100 copay + 20% coinsurance
$25 copay + 20% coinsurance
50% after deductible (limited to $350/day)
50% after deductible (limited to $350/day)
Inpatient Hospitalization
$100 copay per admit + 20%
coinsurance
50% after deductible (limited to $600/day)
Outpatient Surgery
20% after deductible
50% after deductible (limited to $350/day)
Emergency Room
$100 copay + 20% coinsurance
Pharmacy Deductible
Incorporated in Plan Deductible
(must meet deductible before prescription copay applies)
Prescription Drugs
Generic
Preferred Brand
Non-Preferred Brand
Specialty Drugs
$10 copay
$25 copay
$40 copay
20% up to $200 per prescription
$10 copay after plan deductible + 25%
$25 copay after plan deductible + 25%
$40 copay after plan deductible + 25%
20% up to $200 per prescription
Mail Order Pharmacy
Generic
Preferred Brand
Non-Preferred Brand
$20 copay
$50 copay
$80 copay
Not Covered
Not Covered
Not Covered
1
There is an individual deductible within the family deductible. Blue Shield will pay benefits for any family member who
meets the individual medical deductible before the family medical deductible is met.
2
There is an individual out-of-pocket maximum within the family and any family member who meets the individual out-of-
pocket maximum will receive 100% benefits for covered services once the respective out-of-pocket maximum is met.
Page | 9