














 10 / 15
10 / 15

EDM, Inc.
9
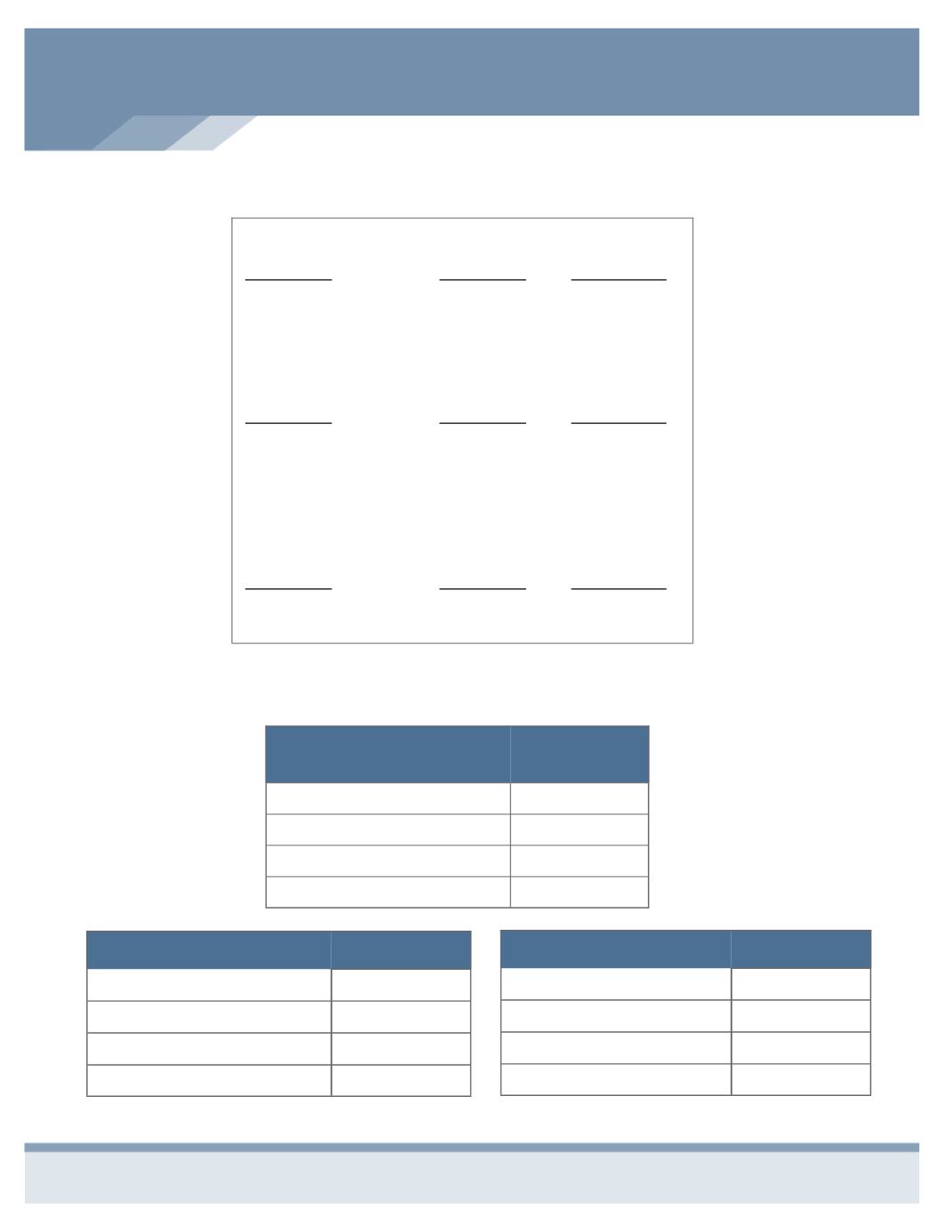
EMPLOYEE COST PER PAY PERIOD
Medical
Bi-Weekly
Deduction
Employee
$0
Employee & Spouse
$322.21
Employee & Child(ren)
$263.63
Family
$617.47
Dental
Employee
$0
Employee & Spouse
$21.35
Employee & Child(ren)
$28.56
Family
$49.92
Employee
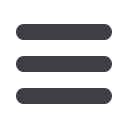
$__________ ÷ 1,000 X $__________ = $___________
Amount of
Coverage
Unit Cost from
Rate Table
Employee
Monthly Cost
Spouse
$__________ ÷ 1,000 X $__________ = $___________
Amount of
Coverage
Unit Cost from
Rate Table
Spouse Monthly
Cost
Child(ren)
$__________ ÷ 1,000 X $__________ = $___________
Amount of
Coverage
Unit Cost from
Rate Table
Child(ren)
Monthly Cost
How to Calculate Your Voluntary Life Premium
Vision
Employee
$0
Employee & Spouse
$2.56
Employee & Child(ren)
$2.85
Family
$5.52