














 4 / 14
4 / 14

4 |
Page
MEDICAL BENEFITS
ABC Company’s medical options are designed to provide you and your family with access to high
quality healthcare. We are offering two plans which are available through UnitedHealthcare. The first
option is a Preferred Plan and the second is the Premier Plan.
The medical options cover a broad range of healthcare services and supplies, including prescriptions,
office visits and hospitalizations. The plans differ when it comes to how they share costs with you.
Please refer to the summary on Page 2 for specific details on each medical plan option.
www.uhc.com.Eligibility:
First of the month following 90 days of employment.
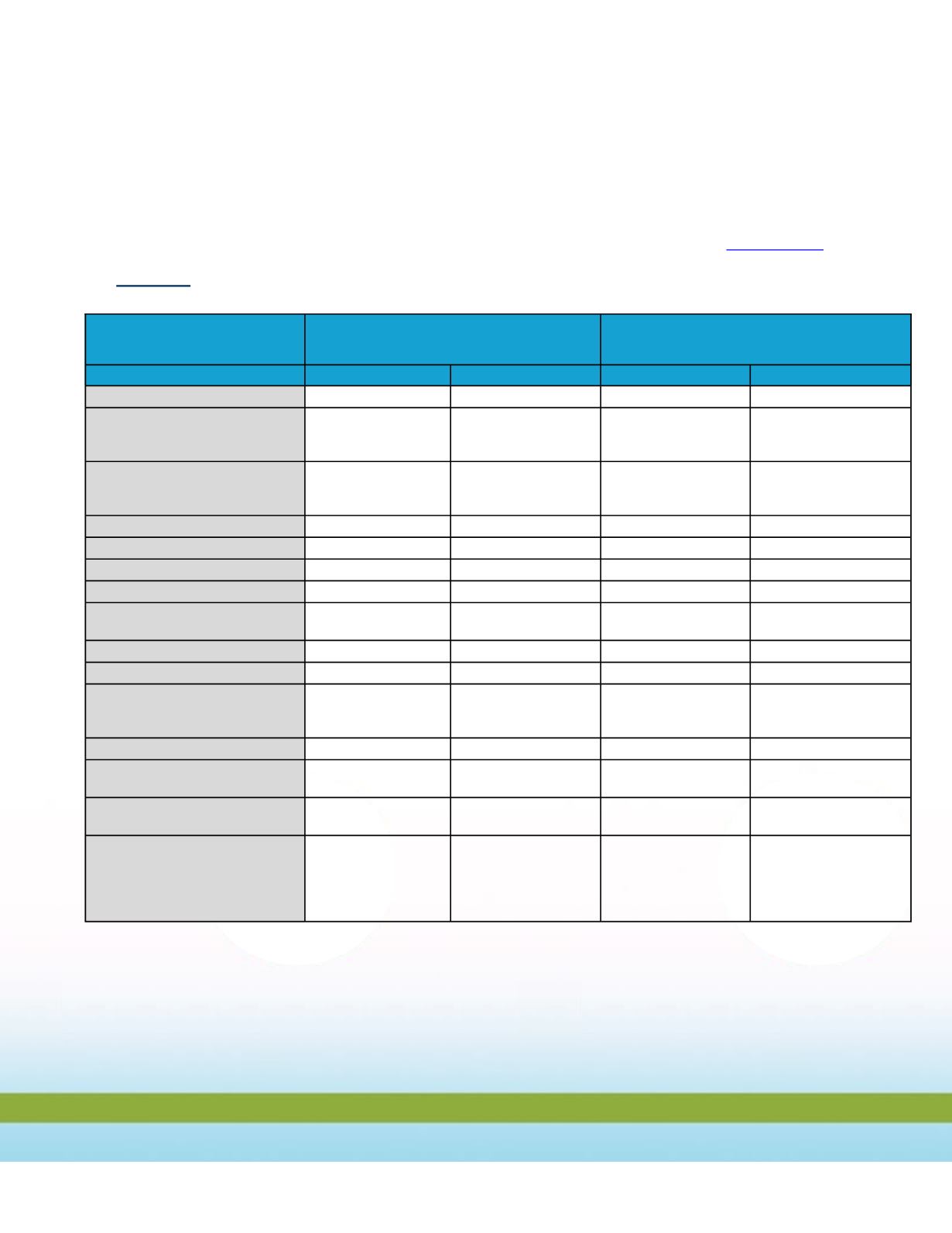
Benefits Description
UnitedHealthcare
PREFERRED - PLAN
UnitedHealthcare
PREMIER - PLAN
In-Network
Out-Of-Network
In-Network
Out-Of-Network
Lifetime Maximum
None
$1 Million
None
$1 Million
Out-Of-Pocket Maximum
Individual
Family
None
None
$5,000
$15,000
None
None
$5,000
$15,000
Deductible
Individual
Family
None
None
$500
$1,500
None
None
$500
$1,500
Coinsurance
100%
70% / 30%
100%
70% / 30%
Primary Office Visit
$20 Copayment
30% after Deductible
$15 Copayment
30% after Deductible
Specialist Services
$40 Copayment
30% after Deductible
$30 Copayment
30% after Deductible
Emergency Room
$100 Copayment
$100 Copayment
$100 Copayment
$100 Copayment
Inpatient Hospital Services
$125/day; to max. of
$625/Admission
30% after Deductible
$125/day; to max. of
$625/Admission
30% after Deductible
Outpatient Surgery
100%
30% after Deductible
100%
30% after Deductible
Lab & Pathology Services
100%
30% after Deductible
100%
30% after Deductible
X-Ray Services
Routine Radiology/Diagnostic
MRI/MRA, CT, PET Scans
100%
100%
30% after Deductible
30% after Deductible
100%
100%
30% after Deductible
30% after Deductible
Routine Mammography
100%
30% after Deductible
100%
30% after Deductible
Routine Eye Exam
(once every other year)
$20 Copayment
30% after Deductible
$15 Copayment
30% after Deductible
Durable Medical Equipment
100%;
$2,500 Max. Benefit
30% after Deductible
100%;
$2,500 Max. Benefit
30% after Deductible
Prescription Drug
(including oral contraceptives)
Generic
Brand
Formulary
$10 Copayment
$30 Copayment
$50 Copayment
$10 Copayment
$20 Copayment
$35 Copayment