















 8 / 21
8 / 21

SCI Engineering, Inc.
5
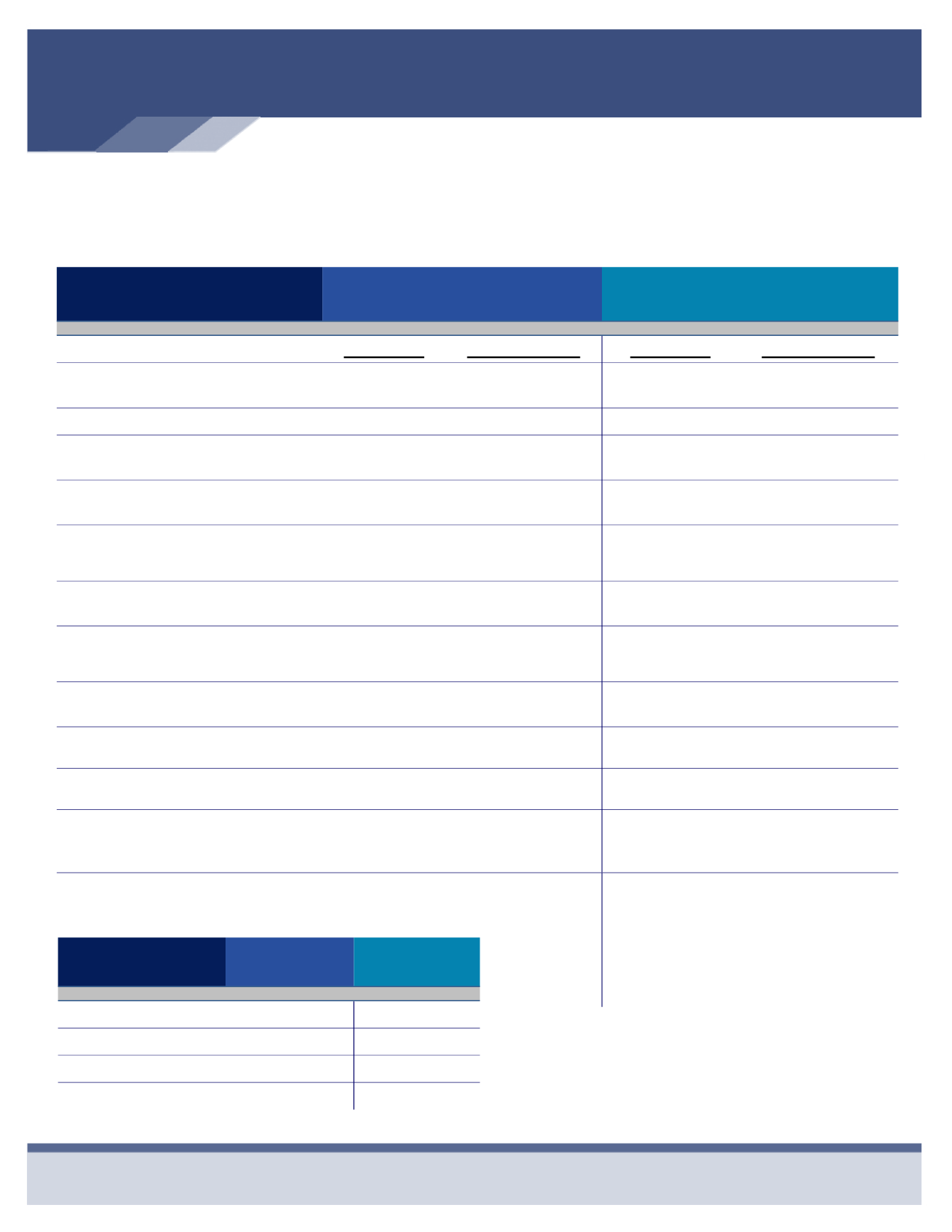
Medical Insurance
UnitedHealthcare - Plan Designs
Features
Traditional PPO Plan
Qualified High
Deductible Health Plan (QHDHP)
HSA Eligible*
In-Network
Out-of-Network
In-Network
Out-of-Network
Deductible
(Individual / Family)
$500 / $1,000
$1,000 / $2,000
$2,600 / $5,200
$5,000 / $10,000
Coinsurance
80%
60%
100%
80%
Out-of-Pocket Maximum
(Individual / Family)
$4,500 / $9,000 $10,000 / $20,000 $5,000 / $10,000
$10,000/ $20,000
Office Visit Co-Pay
(Primary Care physician / Specialist)
$30 / $50
60%
After the Deductible
$30 / $60
After the Deductible
80%
After the Deductible
Preventive Care
100%
Deductible Does Not
Apply
60%
After the Deductible
100%
Deductible Does
Not Apply
80%
After the Deductible
Inpatient Hospital
Outpatient Surgery
80%
After the Deductible
60%
After the Deductible
100%
After the Deductible
80%
After the Deductible
Lab, X-Ray (Outpatient)
100%
Deductible Does Not
Apply
60%
After the Deductible
100%
After the Deductible
80%
After the Deductible
Major Diagnostics (CT, PET, MRI,
MRA, & Nuclear Medicine)
80%
After the Deductible
60%
After the Deductible
100%
After the Deductible
80%
After the Deductible
Emergency Room
$150 Co-Pay
$150 Co-Pay
$300 Co-Pay
After the Deductible
80%
After the Deductible
Urgent Care
$75 Co-Pay
60%
After the Deductible
$75 Co-Pay
After the Deductible
80%
After the Deductible
Prescription Drug
Retail
Mail Order (90-Day Supply)
Tier 1/Tier 2/Tier 3
$10/$30/$50
$25/$75/$125
Tier 1/Tier 2/Tier 3
$10/$30/$50
Not Covered
Tier 1/Tier 2/Tier 3
$10/$30/$50
$25/$75/$125
Tier 1/Tier 2/Tier 3
$10/$30/$50
Not Covered
* If you elect the QHDHP, you may also
participate in the Health Savings Account
(HSA). SCI will contribute $1,000 for indi-
vidual and $2,000 for family coverage to
your HSA on an annual basis. The SCI
contribution is divided and paid on a per
pay period basis.
Per Paycheck Employee Cost
Type of Coverage
Traditional
PPO Plan
QHDHP
Employee
$61.34
$30.41
Employee & Spouse
$208.14
$130.76
Employee & Child(ren)
$175.24
$112.51
Employee & Family
$339.96
$203.73