














 6 / 32
6 / 32

5
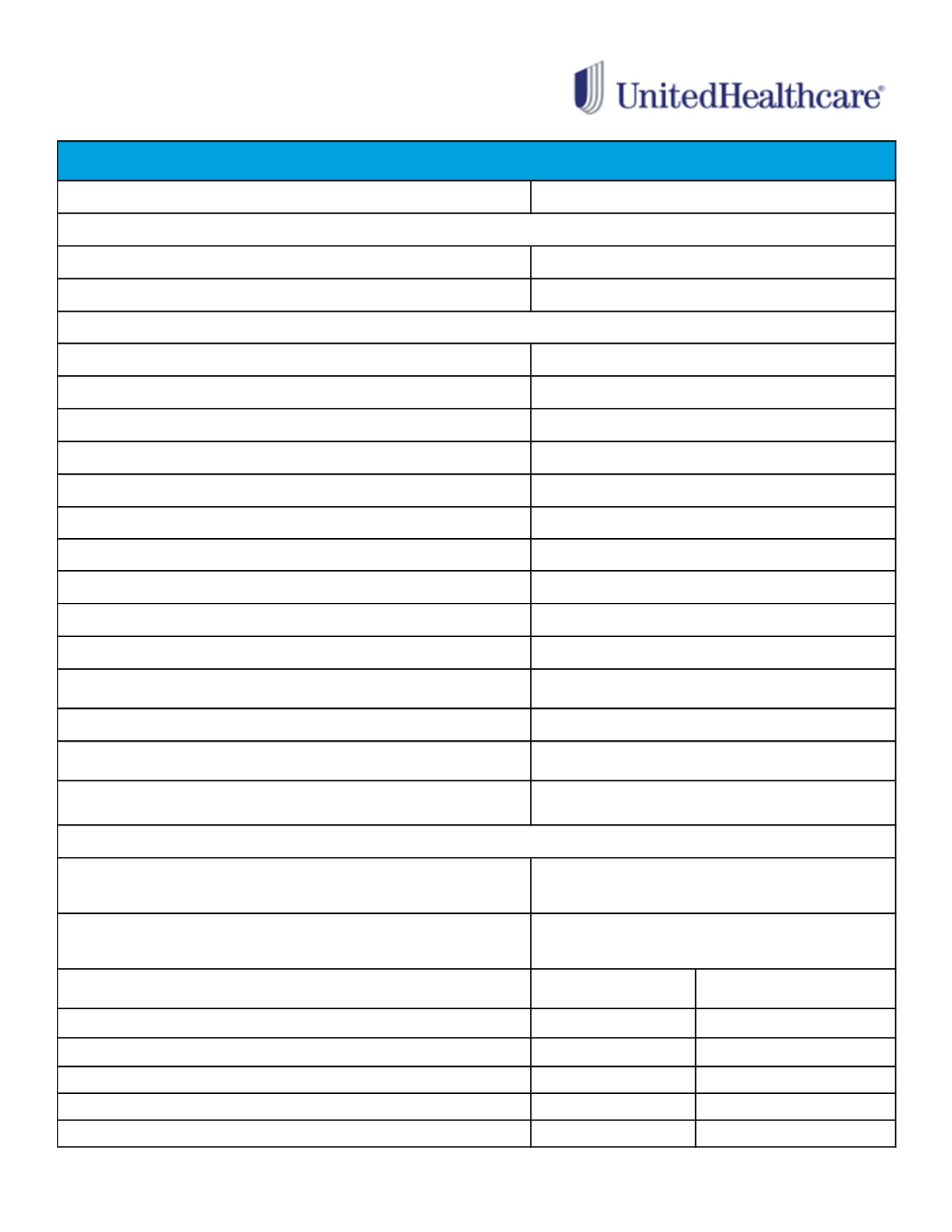
UNDERS TAND I NG
YOUR MEDICAL PLAN
BENEFIT
Individual
Family
Individual
Family
Lifetime Maximum Benefit
Primary Care Physician Office Visits
Specialist Office Visits
Urgent Care Center
Emergency Room
Maternity Physician Services
Hospital Inpatient Expenses
Hospital Outpatient Expenses
Outpatient Therapies
(ex: physical, speech and occupational)
60 visit maximum per calendar year
Chiropractic Care
Mental Health/Behavioral Treatment Services
Durable Medical Equipment
Limited to 1 type of DME (including repair/replacement) every 3 years
Retail Pharmacy
(31 day supply)
Mail Order Maintenance Drug
(90 day supply)
Semi - Monthly Contributions
Pre Tax
Post Tax
Employee
$64.73
$0.00
Employee + 1
$124.65
$0.00
Family
$195.05
$0.00
Domestic Partner (DP)*
$0.00
$59.92
DP & DP Child(ren)*
$0.00
$130.32
$50 co-pay per visit
$100 co-pay (Waived if admitted)
$20 co-pay (First office visit only)
$500 co-pay per inpatient stay
$1,250
$3,750
Unlimited
$20 co-pay per visit
$40 co-pay per visit
CHOICE PLUS BASE PLAN
Annual Deductible
Annual Out of Pocket Maximum
(Includes all co-pays)
IN-NETWORK ONLY
None
None
$10 for Tier 1 drugs
$30 for Tier 2 drugs
$50 for Tier 3 drugs
$25 for Tier 1 drugs
$75 for Tier 2 drugs
$125 for Tier 3 drugs
*In addition to the post tax contributions, a portion of the premium for DP and dependents of DP will be taxable income to the employee. These amounts are
$277.26 for DP coverage only and $494.24 for DP and dependent coverage (per semi monthly pay period).
Plan pays 100%
$20 co-pay
$20 co-pay
Inpatient: $500 co-pay per inpatient stay
Outpatient Services: $20 co-pay per visit
Plan pays 100%
Prescription Drugs