














 3 / 20
3 / 20

P A G E 3
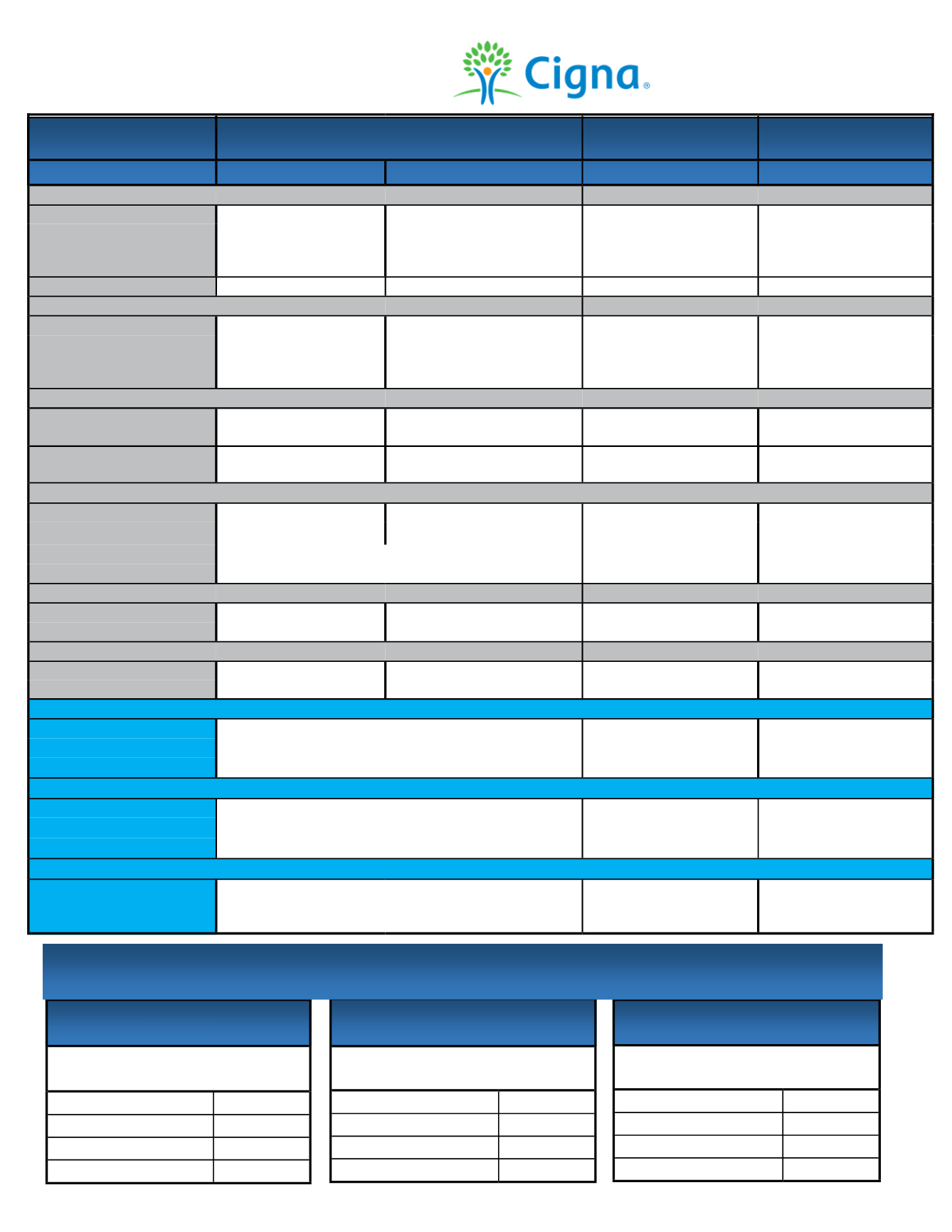
Medical Benefits Description
This spreadsheet is for highlight purposes only. See certificate of coverage for details and limitations.
Plan Design
Open Access Plus Plan
Open Access Plus
In-Network Only Plan
HSA Open Access Plus
In-Network Only Plan
In-Network
Out-of-Network
In-Network
In-Network
Plan Year Deductible
Single
$500
$500
$500
$1,500
Family
$1,000
$1,000
$1,000
$3,000
(combined medical/
prescription)
Coinsurance
Deductible, then no charge
Deductible, then 20%
Deductible, then 20%
Deductible, then no charge
Medical Out-of-Pocket Maximum
Single
$2,500
$2,500
$2,500
$3,000
Family
$5,000
$5,000
$5,000
$6,000
(combined medical/
prescription)
Pharmacy Out-of-Pocket Maximum
Single
$3,500
N/A
$3,500
N/A
Family
$7,000
$7,000
Preventive Care
$0
Birth-Age 16 - 20%, no deductible
Age 17 plus-Deductible, then 20%
$0
$0
Physician Services
Primary Care Physician
$30 Copay
Deductible, then 20% Copay
$30 Copay
Deductible, then no charge
Specialist
$40 Copay
Deductible, then 20% Copay
$40 Copay
Deductible, then no charge
Urgent Care
Deductible, then $40 Copay
Deductible, then $50 Copay
Deductible, then no charge
Emergency Care
Deductible, then $100 Copay
Deductible, then $100 Copay Deductible, then no charge
Outpatient
Lab and x-ray
Deductible, then no charge
Deductible, then 20%
Deductible, then 20%
Deductible, then no charge
Advanced Radiology
Deductible, then no charge
Deductible, then 20%
Deductible, then 20%
Deductible, then no charge
Hospitalization
Inpatient
Deductible, then no charge
Deductible, then 20%
Deductible, then 20%
Deductible, then no charge
Outpatient
Deductible, then no charge
Deductible, then 20%
Deductible, then 20%
Deductible, then no charge
In-Network Prescription Drugs Retail (Up to 90-day supply) * Delaware Residents Please Refer to Summary of Benefits
Generic
You pay $10
You pay $10
Deductible, then you pay $10
Preferred Brand
You pay $25
You pay $25
Deductible, then you pay $25
Non-Preferred Brand
You pay $45
You pay $45
Deductible, then you pay $45
In-Network Prescription Drugs Home Delivery (90-day supply) * Delaware Residents Please Refer to Summary of Benefits
Generic
You pay $20
You pay $20
Deductible, then you pay $20
Preferred Brand
You pay $50
You pay $50
Deductible, then you pay $50
Non-Preferred Brand
You pay $90
You pay $90
Deductible, then you pay $90
Out-of-Network Prescription Drugs * Delaware Residents Please Refer to Summary of Benefits
Pharmacy Deductible
Individual—$50
Family—$100
Deductible, then 20%
Not covered
Not covered
PAYROLL DEDUCTIONS
PER PAY PERIOD
Open Access Plus Plan
Employee
$126.24
Employee + Child(ren)
$391.90
Employee + Spouse
$509.97
Employee + Family
$716.59
PAYROLL DEDUCTIONS
PER PAY PERIOD
Open Access Plus
In-Network Only Plan
Employee
$61.92
Employee + Child(ren)
$279.54
Employee + Spouse
$376.26
Employee + Family
$541.20
PAYROLL DEDUCTIONS
PER PAY PERIOD
HSA Open Access Plus
In-Network Only Plan
Employee
$37.05
Employee + Child(ren)
$212.74
Employee + Spouse
$290.82
Employee + Family
$427.47
Medical Plan Contributions