















 6 / 19
6 / 19

3
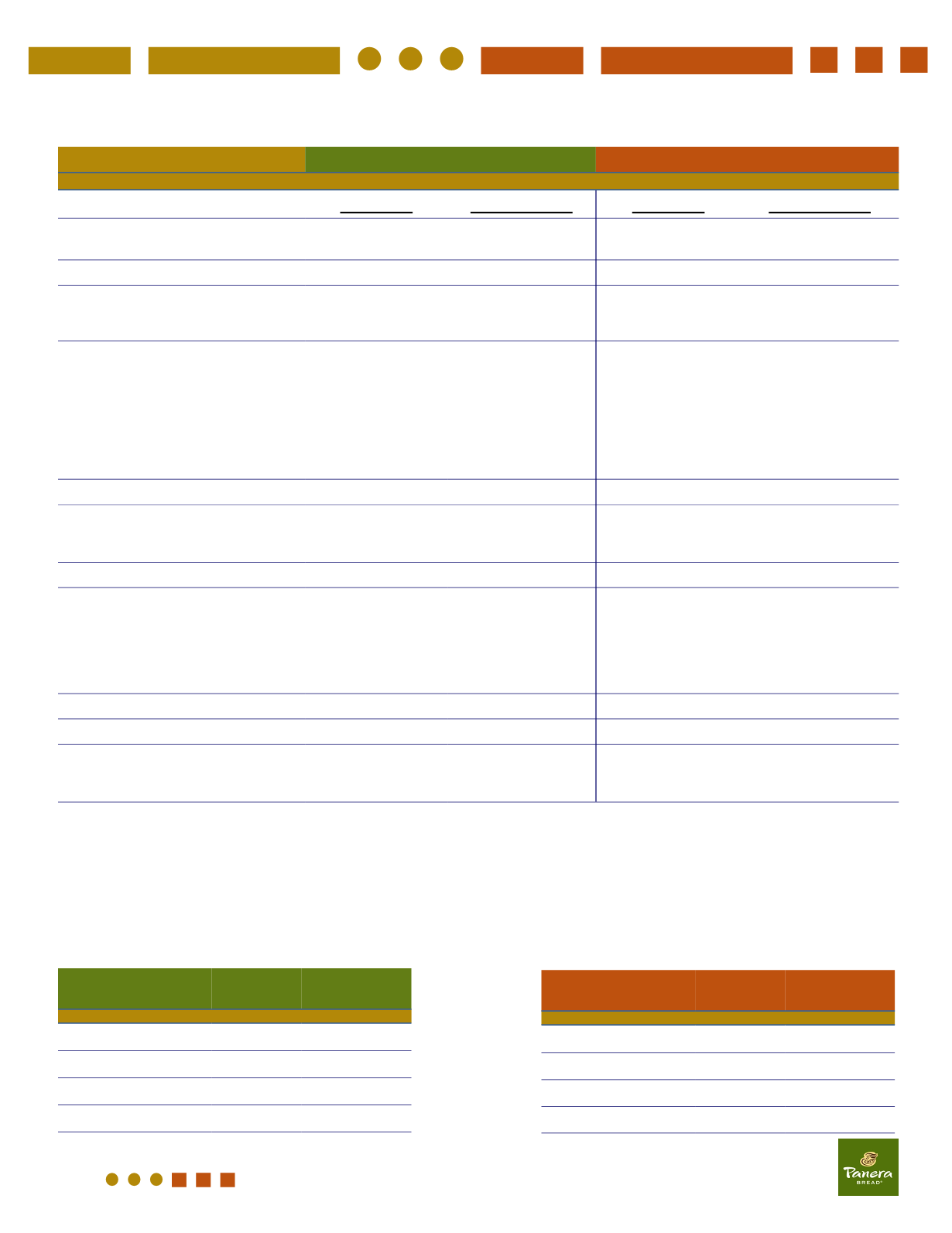
Below are the semi-monthly costs associated with each of the two medical plan options being offered for 2016-2017. If you participate
in the BOTW Wellness program, you are eligible for the reduced semi-monthly premium.
United Healthcare - Plan Designs
Features
Base Plan
Buy-Up Plan
In-Network
Out-of-Network
In-Network
Out-of-Network
Deductible
(Individual / Family)
$3,000 / $6,000
$9,000 / $18,000
$2,000 / $4,000
$4,000 / $8,000
Coinsurance
80%
50%
80%
50%
Out-of-Pocket Maximum
Incl. Co-pays, Coinsurance & Deductibles)
(Individual / Family)
$6,350 / $12,700
$12,500 / $25,000
$6,350 / $12,700
$13,700 / $27,400
Office Visit Co-Pays
(Primary Care physician / Specialist/
Virtual Visits)
$30 / $60 co-pay for
first 4 visits* in a
calendar year; 80%
after deductible for
any subsequent vis-
its in that calendar
year; $30 co-pay for
Virtual Visits**
50% after deductible
$20 / $40 co-pay;
$20 co-pay for
Virtual Visit
50% after deductible
Wellcare Benefits
100%
50% after deductible
100%
50% after deductible
Diagnostics
Lab & X-Ray:
Imaging: (CT, PET, MRI, MRA…)
80% after deductible
80% after deductible
50% after deductible
50% after deductible
80% after deductible
80% after deductible
50% after deductible
50% after deductible
Emergency Room
80% after In-Network deductible
$150 Co-pay
Urgent Care
$75 co-pay for first 4
visits in a calendar
year; 80% after
deductible for any
subsequent visits in
that year
50% after deductible
$100 Co-pay
50% after deductible
Hospital - Inpatient Stay
80% after deductible 50% after deductible 80% after deductible
50% after deductible
Surgery Outpatient
80% after deductible 50% after deductible 80% after deductible
50% after deductible
Prescription Drug
Retail
Mail Order (90-Day Supply
)
at Participating Pharmacies
$10 / $35 / $70 Co-Pay
$25 / $87.50 / $175 Co-Pay
at Participating Pharmacies
$10 / $35 / $70 Co-Pay
$25 / $87.50 / $175 Co-Pay
*Wellness visits do not count toward your 4 plan office visit maximum per year.
**Virtual Visits do not count toward your 4 office visit maximum per calendar year. You have unlimited availability to
Virtual Visits.
Base Plan Semi- Monthly
Employee Cost
Type of Coverage
Cost With
Wellness
Cost Without
Wellness
Employee
$79.00
$124.90
Employee & Spouse
$204.48
$265.82
Employee & Child(ren)
$184.78
$240.21
Employee & Family
$282.23
$366.89
Buy-Up Plan Semi-Monthly
Employee Cost
Type of Coverage
Cost With
Wellness
Cost Without
Wellness
Employee
$138.98
$180.68
Employee & Spouse
$292.34
$380.05
Employee & Child(ren)
$264.65
$344.05
Employee & Family
$403.64
$524.73