
















 2 / 2437
2 / 2437

07.11.2017
2
Proposed format & overarching goal
7
• Layer 1: Morphological classification
• Layer 2: WHO grade (reflects natural tumor history)
• Layer 3: Molecular information
Integrated diagnosis
• Adds a level of objectivity to the diagnostic process
• Stratifies tumors into biologically homogenous groups
• Enhances diagnostic accuracy & prognostic rating
CAVE
Diagnostic
delay
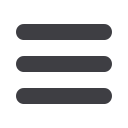
Community Surveys (SNO & ISN)
8
NeuroOncol. 2016;19:336-344.
Surveys provided overwhelmingly
positive feedback
Classification based on histology & genetics
9
• International collaboration of 117 contributors from 20 countries
• Three-day consensus conference by a working group of 35
neuropathologists, clinical advisors and scientists from 10
countries
Austrian contributors:
Johannes A. Hainfellner
Matthias Preusser
How many brain tumor entities are
differentiated according to the WHO 2016
classification?
10
• A1. 1-30
• A2. 40-70
• A3. 80-110
• A4. 120+
A4 is correct
11
12
2016
2007
Diffuse astrocytomas more similar to
oligodendrogliomas than pilocytic
astrocytomas -> family trees redrawn
Diffuse astrocytoma categories:
IDH-mutant
IDH-wildtype
NOS
WHO grading II-III retained
Gliomatosis cerebri deleted (invasive
growth of diffuse astrocytoma,
oligodendroglioma or glioblastoma)
Molecular markers now mandatory
IDH, 1p19q, H3K27