
















 10 / 32
10 / 32

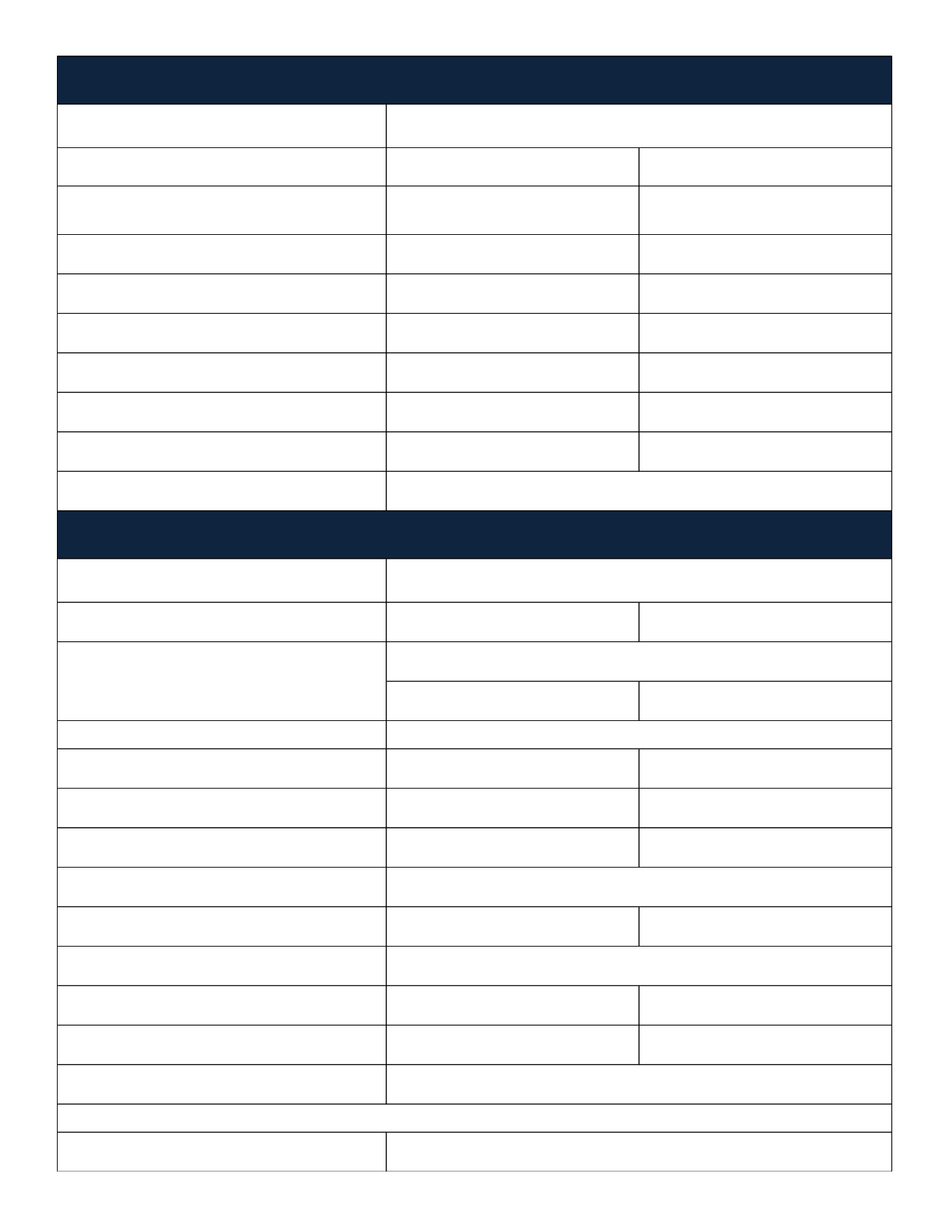
Type of Plan
In-Network
Out-of-Network
(Non-Participating providers can bill
you for charges above amount covered
by your HumanaDental plan)
Deductible
Single: $50
Family: $150
Single: $50
Family: $150
Annual Maximum Benefit
$1,000
$1,000
Preventive Services
(oral exam, cleaning, bitewing x-rays)
100%
100%
Basic Services
(fillings, simple extractions, other x-rays)
80% after Deductible
80% after Deductible
Major Services
(crowns, dentures, oral surgery, root canals)
50% after Deductible
50% after Deductible
Orthodontia
Not Covered
Not Covered
Contact Information
Type of Plan
Network Providers include: Costco, Visionworks, plus
private practitioners
In-Network
Out-Of-Network
$20 Copay
$35 Allowance
Eyeglass Lenses
Single Vision
$20 Copay
$33 Allowance
Bifocal
$20 Copay
$50 Allowance
Trifocal
$20 Copay
$65 Allowance
Frames
$40 Wholesale Allowance
$57 Retail Allowance
Contact Lenses (in lieu of frames or glasses)
Elective (Conventional & Disposable)
$110 Allowance
$110 Allowance
Medically Necessary (limit one pair)
100%
$280 Allowance
Additional Discounts
Contact Information
Voluntary Dental Coverage
HumanaDental - Voluntary - Traditional Preferred 09
Voluntary Vision Coverage
HumanaVision - Voluntary - Vision Care Plan
1.800.233.4013
www.humana.comOnce per 12 months
Examination
1.866.537.0229
www.HumanaVisionCare.com20% discount on additional pair of glasses or frames, see plan summary for details.
Discounts on LASIK, see plan summary for details.
Once per 12 months
Once per 24 months
Once per 12 months