















 8 / 31
8 / 31

Donald Danforth Plan Science Center
5
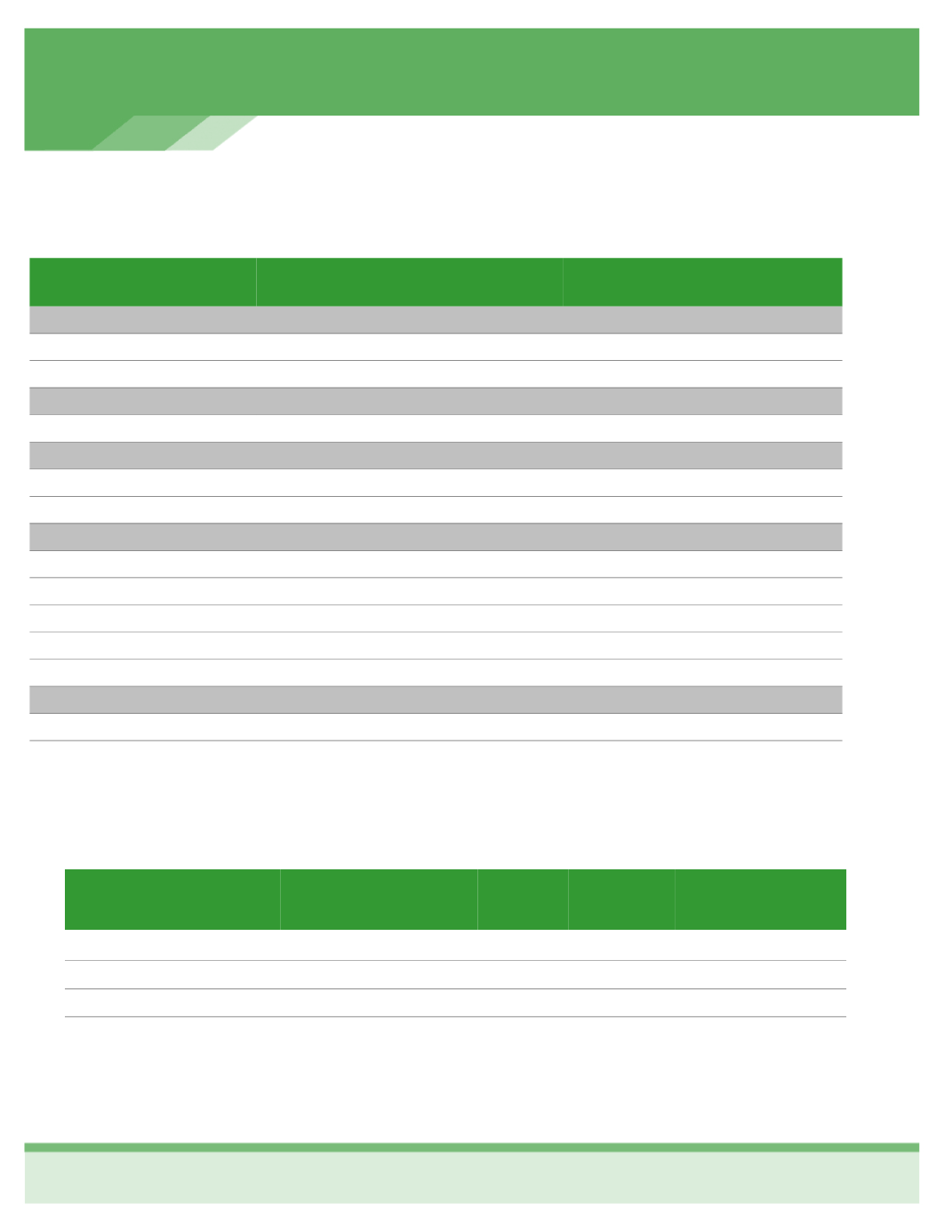
MEDICAL INSURANCE
UnitedHealthcare Medical
Benefit Plan—Enhanced Plan
In Network
Out of Network
Deductible
(calendar year)
Single
$250
$500
Family
$500
$1,000
Coinsurance
(plan pays/you pay)
100% / 0%
80% / 20%
Out of Pocket Limit
(including the deductible + coinsurance + copayments)
Single
$3,500
$5,300
Family
$7,000
$10,000
Copayments
Primary Physician Visit
$20 co-pay
Deductible, then you pay 20%
Specialist Physician Visit
$40 co-pay
Deductible, then you pay 20%
Preventive Care
Plan pays 100%
Deductible, then you pay 20%
Emergency Room Visit
$200 co-pay
$200 co-pay
Urgent Care Center Visit
$50 co-pay
Deductible, then you pay 20%
Prescription Drug Coverage
Retail Pharmacy
$10/35/60
$10/35/60
Mail Order Pharmacy
$25/87.50/150
$25/87.50/150
2016 Employee Enhanced Plan Medical and Dental Contributions
Employee Deduction (for
Medical and Dental per
pay period)
Total
The
Center
Pays
Employee
Monthly
Cost
Employee
Per Pay
Period Cost
Employee Per Pay
Period Cost with
Spousal Surcharge
Employee
$540.10
$432.10
$108.00
$54.00
$54.00
Employee & Spouse
$1,130.83
$858.83
$272.00
$136.00
$161.00
Employee & Child(ren)
$1,046.13
$794.13
$252.00
$126.00
$126.00
Employee & Family
$1,593.21
$1,179.21
$414.00
$207.00
$232.00