















 6 / 12
6 / 12

6
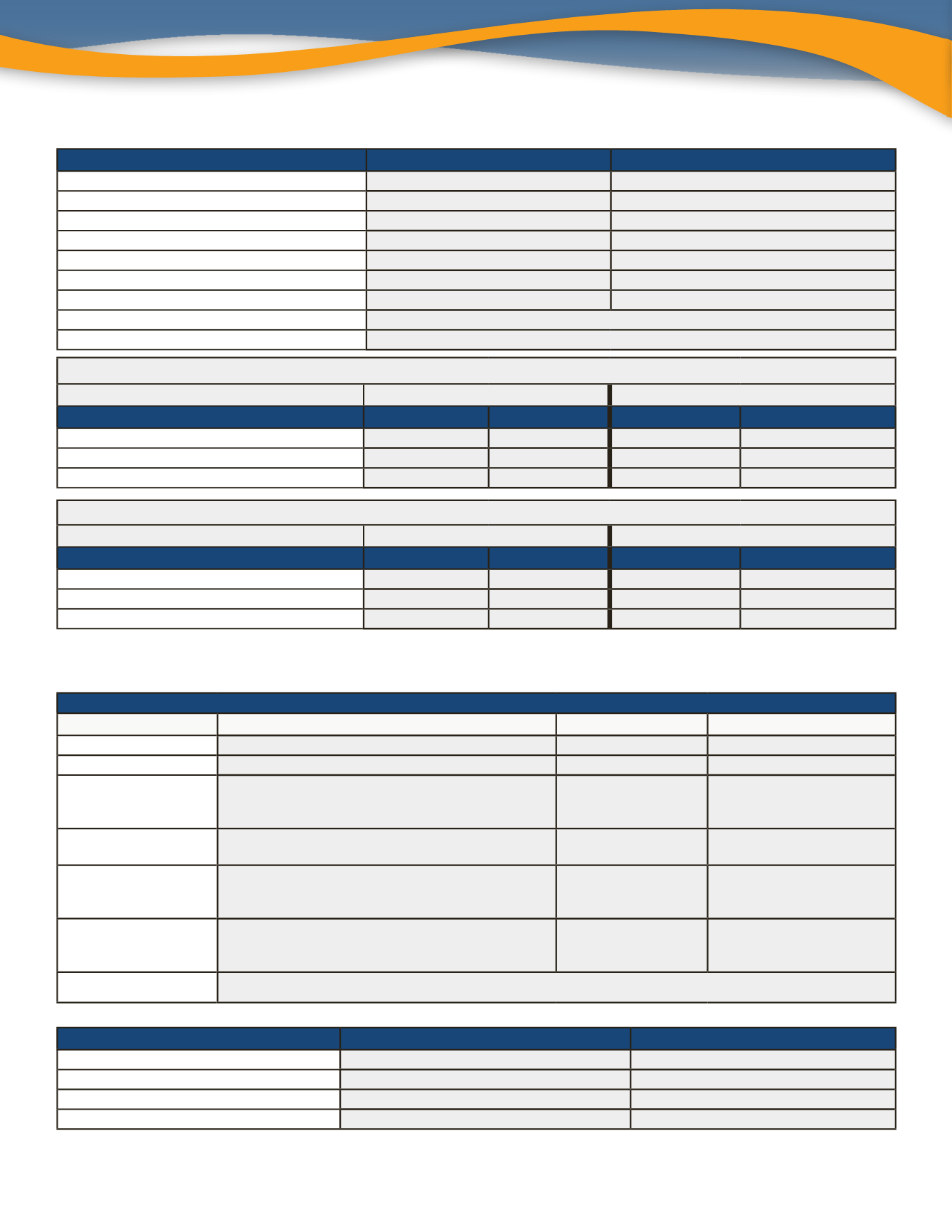
In-Network Benefits
AMERITAS - Low Plan
AMERITAS - High Plan
Annual Maximum
$1,000
$2,500
Deductible - Waived for preventive
$50 / $150
$50 / $150
Preventive
100%
100%
Basic
80%
90%
Major
25%
60%
Orthodontia Coinsurance
N/A
50% - Child Only
Orthodontia Maximum
N/A
$2,500 (Lifetime)
Dental Rewards Program
Additional accumulation toward annual maximum
FUSION Benefit
$100 to use for eye exams, frames and lenses
Full Time Employees Working 30+ Hours Per Week
Low Plan
High Plan
RATES
Employee Per Month EmployeePer Paycheck Employee Per Month Employee Per Paycheck
Employee Only
$12.00
$6.00
$30.00
$15.00
Employee + One
$28.00
$14.00
$54.00
$27.00
Employee + Family
$50.00
$25.00
$96.00
$48.00
Part Time Employees Working 20-29 Hours Per Week
Low Plan
High Plan
RATES
Employee Per Month EmployeePer Paycheck Employee Per Month Employee Per Paycheck
Employee Only
$19.00
$9.50
$40.00
$20.00
Employee + One
$35.00
$17.50
$70.00
$35.00
Employee + Family
$58.00
$29.00
$120.00
$60.00
Participants have 90 days from the date of service to file a FUSION claim with Ameritas.
Voluntary Vision Plan - VSP
Dental Plans - Ameritas
VSP CHOICE
Description
Copay
Frequency
WellVision Exam
Focuses on your eyes and overall wellness
$10
Every 12 Months
Glasses
Prescription glasses
$25
See Frame and Lenses
Frames
• $150 allowance for a wide selection of frames
• $80 allowance at Costco
• 20% off amount over your allowance
Included in prescription
glasses
Every 24 Months
Lenses
• Single vision, lined bifocal and lined trifocal lenses
• Polycarbonate lenses for dependent children
Included in prescription
glasses
Every 12 Months
Lens Options
• Standard progressive lenses
• Premium progressive lenses
• Custom progressive lenses
$55
$95 - $105
$150 - $175
Every 12 Months
Contacts
(instead of glasses)
• $150 allowance for contacts and contact lens exam
(fitting and evaluation)
• 15% off contact lens exam (fitting and evaluation)
$0
Every 12 Months
FUSION Benefit
$100 to use for exams, frames and lenses
RATES
Employee Per Month
Employee Per Paycheck
Employee Only
$5.91
$2.96
Employee + Spouse
$11.82
$5.91
Employee + Child(ren)
$12.63
$6.32
Employee + Family
$20.19
$10.10