














 41 / 60
41 / 60

 www.speechpathologyaustralia.org.au
www.speechpathologyaustralia.org.au
JCPSLP
Volume 17, Number 1 2015
39
university, six clinicians in total, were invited to participate in
this study via email or phone contact. All six clinicians
accepted (Group A). Invitations were then extended to six
clinicians known to the lead author not to take students and
five accepted (Group B). Consent was obtained from all
participants to be interviewed. Table 1 provides summary
data on interview participants in both groups.
Group A participants had a mean of 8.3 years of
experience (range = 5–11 years) and Group B had a
mean of 18.2 years of experience (range = 12–25 years).
All participants were in private practice as their primary
position. Ten out of the 11 participants were female, which
is similar to the national gender demographic of speech
pathologists (HWA, 2014). Most participants were practice
owners, either in sole trader positions or employers. The
majority provided paediatric services only.
Data collection
The lead author completed an interview with each
participant using a semi-structured interview guide.
Examples of questions include: “Tell me about yourself and
your practice (e.g., years of experience, caseload,
employment status, service deliveries used within the
practice, funding schemes accessed for clients)”; “Tell me
what you see as benefits of having students in your
practice”; “Would you consider taking students in the
future? If yes? – what are the perceived benefits, and
perceived barriers/challenges. If no? – why?” As this was a
scoping study, exploring clinician views and perceptions,
semi-structured interviews were chosen as they are the
most widely used format in qualitative research, allowing
the interviewer to explore more deeply into the issues being
investigated (DiCicco-Bloom & Crabtree, 2006). The
interviews were conducted either face-to-face or over the
phone depending on participant availability. Group A
as clinical coordinators to describe barriers to speech
pathology student placements and identify ways to address
them. They found that allowing clients to choose and
consent to having a student clinician and by maintaining
an “apprenticeship” style of supervision, the positives for
the student, client, and private practitioner outweighed
the negatives. They went on to conclude that student
placements are possible in private practice. However, their
report was based on evaluation of one student’s placement
in one private practice, and did not explore a range of
known barriers to placements in private practice.
A first step in diversifying and increasing student
placements in speech pathology private practice is to
understand the barriers and benefits private practitioners
perceive about supervising students in private practice.
We conducted a quality improvement project with two
groups of private practitioners, those who had previously
supervised students on placement and those who had
not, to explore their views and perceptions of (a) roles
for, barriers to, and benefits associated with student
placements in private practice and (b) satisfaction of
clinicians, parents/clients, and students involved in student
placements in private practice.
Method
This project used semi-structured interviews with two
groups of speech pathologists working in private practice:
those who had supervised student placements and those
who had not.
Recruitment
Convenience sampling was used to recruit speech
pathologists through private practice and university
networks in New South Wales, Australia. All private practice
clinicians known to take students from the authors’
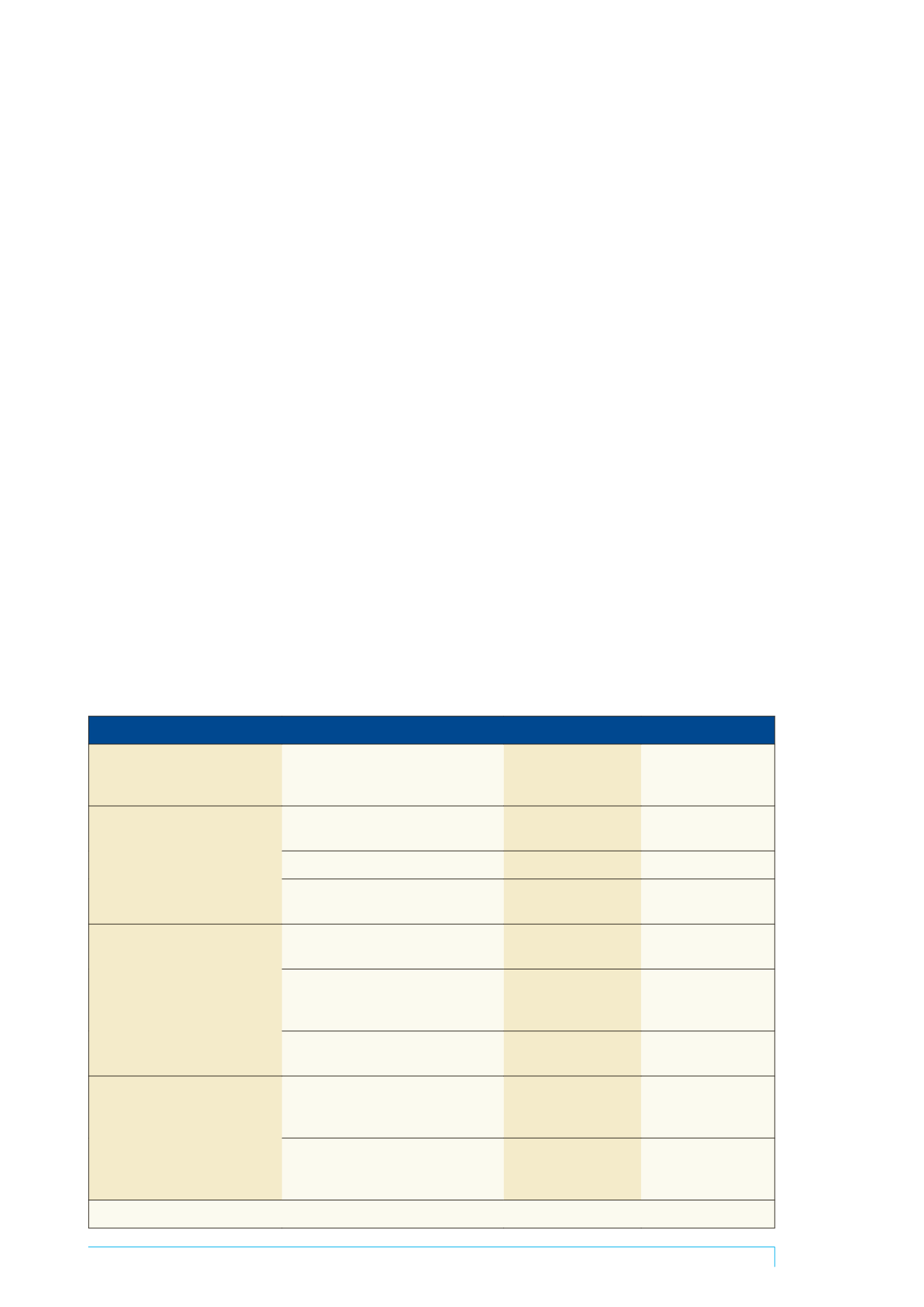
Table 2. Participant identified factors requiring participation of private practices in student placements
Category
Subcategory
Found in Group A: those
who had taken students
on placements
Group B: those who
had not taken students
on placements
Shrinking public sector – growing
private sector
An increase in the number of new graduates
entering in private practice
*
*
NDIS roll out
*
*
Growing waiting lists in community health
and the importance of early intervention
*
*
A need for student exposure to
differing models, service deliveries
and experiences
Limitations to service delivery models exist
in public sector
*
*
Private sector involves many differing
service deliveries and clinical management
approaches and capabilities
*
*
To demonstrate to students a good, ethical
and effective model of private practice
*
*
A need to ensure graduates are work
ready
New graduates need to learn about the
business and administration side of private
practice
*
*
Ever growing legal issues and legislation
around private practice that new graduates
need to know about
*
*
* = found in data from this group