

















 237 / 1082
237 / 1082

S224
ESTRO 36 2017
_______________________________________________________________________________________________
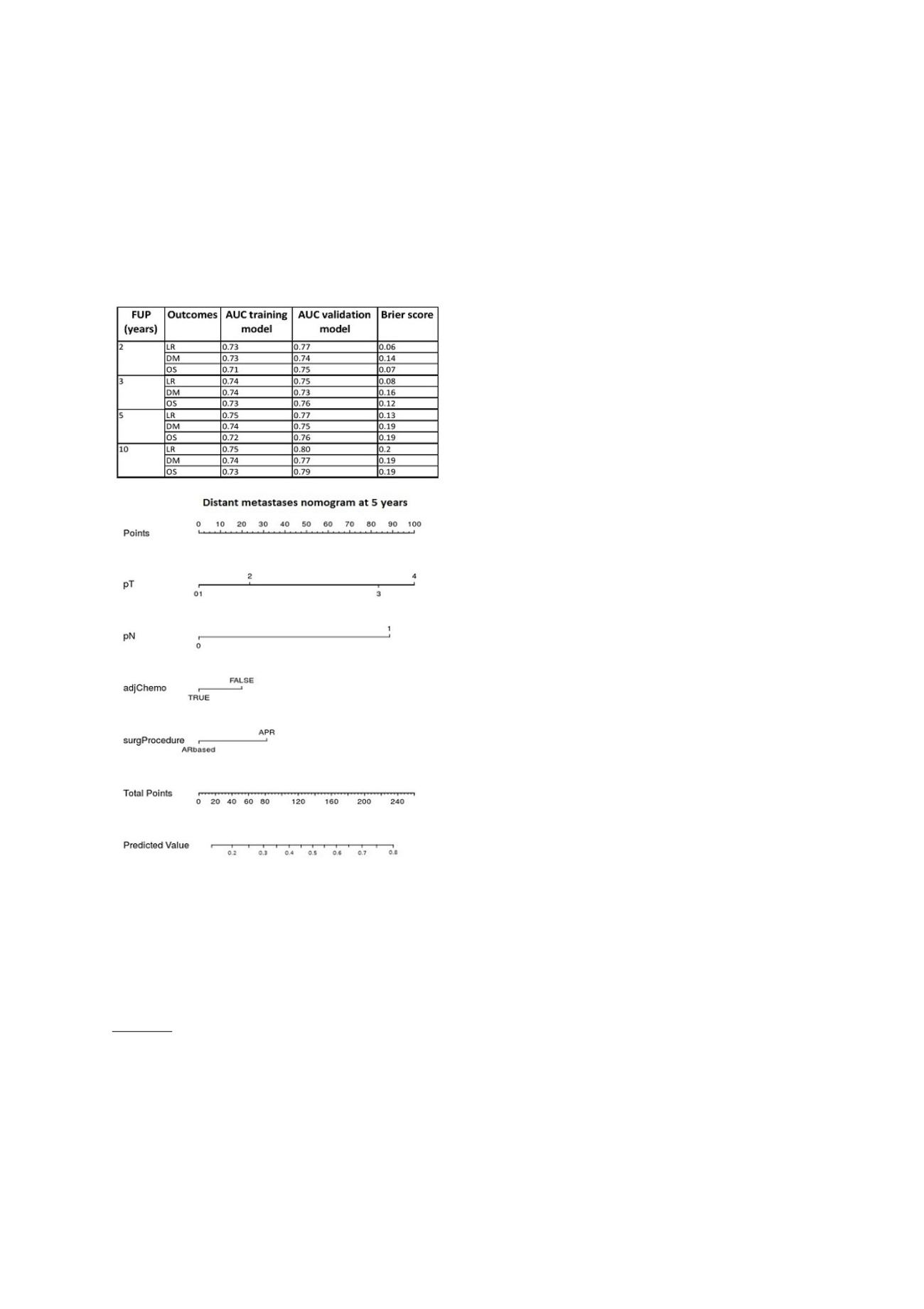
were validated using external validation of type 2b. The
models performance was evaluated using the Area under
the Receiver Operating Curve (AUC) and the brier score.
Results
Three thousand seven hundred seventy patients out of
7612 patients in this pooled dataset satisfied the inclusion
criteria and were analyzed in this study. For each outcome
(LR, DM and OS) performance of training and validation
models, in terms of AUC and brier score were shown in
table 1. Nomograms were generated for each outcome
(LR, DM and OS) at 2, 3, 5 and 10 years. Furthermore as
an example we have reported the new distant metastases
nomogram at 5 years obtained (Figure 1).
Conclusion
The logistic regression models performed with AUC values
always higher than 0.7. The AUC higher in validation than
in training would need further investigation. Nomograms
will be totally showed at the conference.
[1] V. Valentini et al;Journal Clinical Oncology; 2011 [2] S.
Gary et al; Research reporting method; 2015
OC-0428 Surgical time to increase pCR in rectal
cancer: pooled set of 3078 patients from 7 randomized
trials
G. Chiloiro
1
, C. Masciocchi
1
, J. Van Soest
2
, E. Meldolesi
1
,
M. Gambacorta
1
, J. Bosset
3
, J. Doyen
4
, J. Gerard
4
, S.
Ngan
5
, C. Roedel
6
, F. Cellini
1
, A. Damiani
1
, N. Dinapoli
1
,
P. Lambin
2
, A. Dekker
2
, V. Valentini
1
1
Università Cattolica del Sacro Cuore -Policlinico A.
Gemelli, Radiation Oncology Department, Rome, Italy
2
Maastricht University Medical Center, Department of
Radiation Oncology MAASTRO-GROW School for Oncology
and Development Biology, Maastricht, The Netherlands
3
Besançon University Hospital J Minjoz, Department of
Radiation Oncology, Besançon, France
4
Unicancer Centre Antoine Lacassagne, Radiotherapy,
Nice, France
5
Peter MacCallum Cancer Centre, Division of Radiation
Oncology, Melbourne, Australia
6
Goethe University Frankfurt, Department of
Radiotherapy and Oncology, Frankfurt am Main,
Germany
Purpose or Objective
Optimal timing of surgery after neoadjuvant chemo-
radiotherapy (NAD-CRT) is still controversial. Literature
data suggest an improvement in pathological complete
response (pCR) after prolongation of surgical interval (SI)
after NAD-CRT. The aim of this study was to evaluate the
effects of SI on pCR in a pooled dataset of locally advancer
rectal cancer (LARC) patients (pts) coming from 7
randomized trials.
Material and Methods
Pts data were extracted from the following LARC trials:
Accord 12/0405, EORTC 22921, FFCD 9203, CAO/ARO/AIO-
94, CAO-ARO-AIO-04, INTERACT and TROG 01.04. Inclusion
criteria for pts selection were: LARC (clinical tumor stage
(cT) 3-4, clinical nodal stage (cN) 0-1-2 and no distant
metastases) and NAD-CRT followed by surgery. The SI was
calculated from the end of NAD-CRT. Pts were divided into
two groups according to median of the surgery time (MST):
shorter interval group (SIG) (pts who had surgery before
MST) and longer interval group (LIG) (pts who had surgery
after MST). The primary outcome was to determine the
rate of pCR related to SI. The secondary outcome was to
compare post-surgical complications in two groups and the
impact of pCR rates on local recurrence (LR), metastases-
free survival (MFS) and overall survival (OS). Pearson's Chi-
squared test, Kaplan-Meier curves and univariate logistic
regression model (uLRM) were used for data analysis. A p-
value<=0.05 was considered significant.
Results
This pooled dataset included 5247 pts; 3078 pts satisfied
the inclusion criteria and were analyzed in this study.
Recruitment in the period investigated by the study took
place as follows: 453 pts from 1993 to 1998, 613 from 1999
to 2003, 1023 from 2004 to 2008 and 996 from 2009 to
2014. 440 (14%) pts had pCR. The cumulative pCR rate rose
significantly when time between NAD-CRT and surgery was
increased, until reaching a plateau at 16 weeks (Figure 1).
MST was 6 weeks (range 1-31, range interquartile 5-7). The
SIG and the LIG had 1953 and 1132 pts, respectively. pCR
rates were significantly higher in the LIG as compared to
the SIG (19% vs 11.6%, p<0.01). cT, cN, surgery procedure
and post surgical complications were distributed equally
between the two groups. The results of uLRM are
summarized in table 1. Finally, considering only the pCR
events there was no statistically significant difference in
term of LR, MFS and OS between the two groups.
Comparing the two groups, considering pCR and no pCR
pts, there was no statistically significant difference in
term of LR, MFS and OS between them.